
GLP-1 Microdosing in 2026: Why U.S. Patients Do It, What It Really Saves, and A Better Alternative
Key Takeaways
- GLP-1 microdosing involves independent, unapproved dose reductions that completely lack clinical standardization or FDA safety approval.
- Prohibitive retail pricing and intense gastrointestinal issues prompt patients to ration brand-name pens or stretch injection intervals.
- Stricter FDA compounded medication rules are actively phasing out unapproved copies as national supply shortages resolve.
- Subtherapeutic dosing degrades clinical efficacy, which frequently leads to stalled progress, medication waste, or rapid weight regain.
U.S. patients often reduce their weight loss medication doses to manage high costs. Some also try this to limit severe gastrointestinal side effects. However, the true financial impact of GLP-1 microdosing in 2026 remains highly debated. Stretching a prescription compromises your treatment and often stalls clinical progress. Safer, regulated alternatives exist to help you maintain a standard therapeutic dose.
What Is GLP-1 Microdosing and How Does It Differ from Approved Regimens?
GLP-1 microdosing means taking less than the officially prescribed amount of your medication. Patients independently reduce their dose or change their schedule. This unapproved practice lacks clinical testing and formal safety data.
Official regimens follow strict guidelines from the Food and Drug Administration. Doctors start your treatment at a low baseline dose. They gradually increase the amount to a standard therapeutic dose. This controlled process allows your body to adjust safely over time.
The primary difference involves the complete lack of medical oversight. Unofficial microdosing protocols do not achieve verified metabolic thresholds. Comparing microdosing GLP-1 vs. regular dose routines highlights critical health risks. Independent changes bypass the clinical benchmarks required for real medical success.

Why U.S. Patients Are Turning to GLP-1 Microdosing in 2026
High out-of-pocket expenses drive many individuals toward unapproved medication habits. Strict insurance barriers complicate long-term access to brand-name weight loss options. Patients modify their regimens to address critical financial and physiological challenges.
Cost Pressures and Insurance Barriers
The high cost of Ozempic without insurance creates immediate financial hurdles for cash-paying buyers. Retail prices for brand-name formulations regularly exceed one thousand dollars per month. A sudden GLP-1 insurance denial leaves individuals without a viable treatment path. Insurers often require prior authorizations or apply strict clinical criteria for weight management. Patients look for: how to save money on Wegovy by stretching single-pen devices. Rationing doses allows a single prescription to last multiple months.
Managing Gastrointestinal Side Effects
Severe physical discomfort represents another primary driver for independent dose reduction. Standard escalation schedules often cause intense nausea, vomiting, or bloating. Unsupervised adjustments for microdosing GLP-1 side effects are common in online wellness forums. A recent health survey reported that 15% of users explore alternative doses. Roughly 41% of these individuals seek to minimize digestive issues. About one-third of surveyed patients focus purely on immediate financial relief. Patients attempt to maintain weight loss benefits without experiencing debilitating daily symptoms.
Weight Maintenance Strategies
Achieving a goal weight prompts some individuals to lower their weekly medication quantities. Patients try to prevent weight regain while reducing their overall medication burden. Dropping to a fractional amount satisfies their desire for long-term appetite management. However, subtherapeutic doses fail to replicate the data-proven metabolic thresholds. Altering the prescribed plan without direct clinical supervision threatens therapeutic continuity.
Common GLP-1 Microdosing Methods Patients Discuss Online
Patients share several unapproved techniques to modify their clinical treatment plans online. These observational methods bypass standardized medical protocols. They introduce severe accuracy and safety risks to your health.
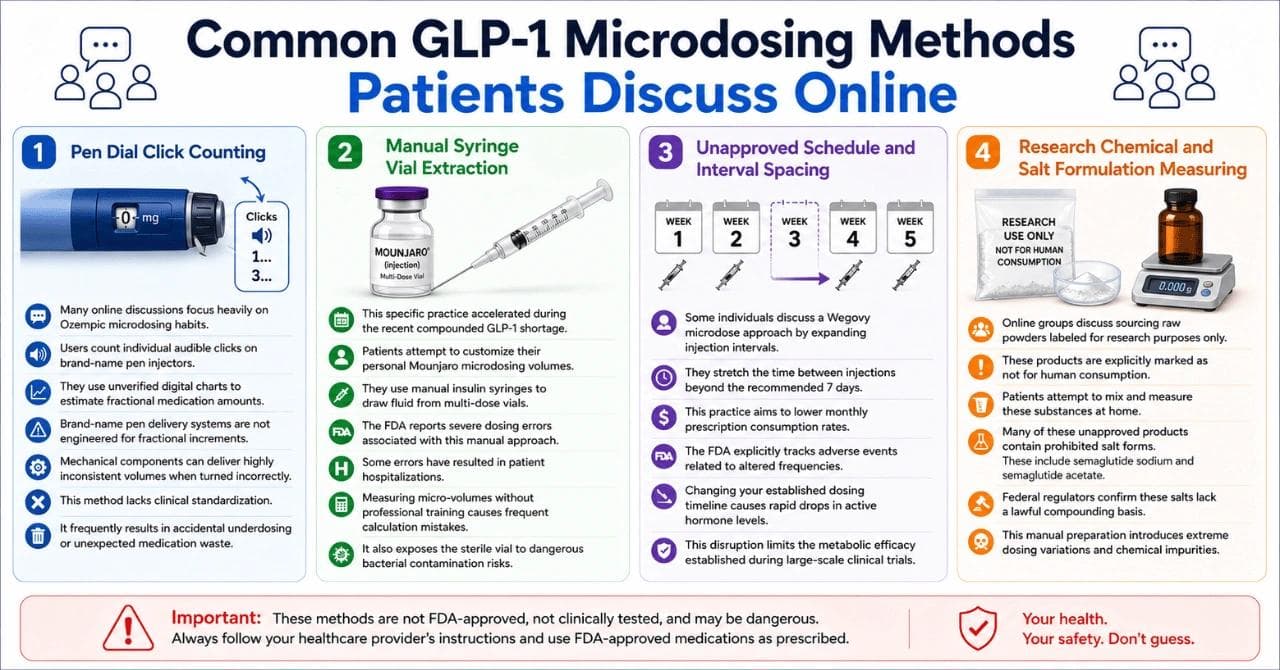
Pen Dial Click Counting
Many online discussions focus heavily on Ozempic microdosing habits. Users count individual audible clicks on brand-name pen injectors. They use unverified digital charts to estimate fractional medication amounts. Brand-name pen delivery systems are not engineered for fractional increments. Mechanical components can deliver highly inconsistent volumes when turned incorrectly. This method lacks clinical standardization. It frequently results in accidental underdosing or unexpected medication waste.
Manual Syringe Vial Extraction
This specific practice accelerated during the recent compounded GLP-1 shortage. Patients attempt to customize their personal Mounjaro microdosing volumes. They use manual insulin syringes to draw fluid from multi-dose vials. The FDA reports severe dosing errors associated with this manual approach. Some errors have resulted in patient hospitalizations. Measuring micro-volumes without professional training causes frequent calculation mistakes. It also exposes the sterile vial to dangerous bacterial contamination risks.
Unapproved Schedule and Interval Spacing
Some狂 individuals discuss a Wegovy microdose approach by expanding injection intervals. They stretch the time between injections beyond the recommended 7 days. This practice aims to lower monthly prescription consumption rates. The FDA explicitly tracks adverse events related to altered frequencies. Changing your established dosing timeline causes rapid drops in active hormone levels. This disruption limits the metabolic efficacy established during large-scale clinical trials.
Research Chemical and Salt Formulation Measuring
Online groups discuss sourcing raw powders labeled for research purposes only. These products are explicitly marked as not for human consumption. Patients attempt to mix and measure these substances at home. Many of these unapproved products contain prohibited salt forms. These include semaglutide sodium and semaglutide acetate. Federal regulators confirm these salts lack a lawful compounding basis. This manual preparation introduces extreme dosing variations and chemical impurities.
How the Compounded GLP-1 Phase-Out Impacts Patient Access in 2026
Federal regulators have shifted enforcement policies regarding unapproved copies of weight management medications. These updates alter the pricing and availability landscape for thousands of American consumers.
- Removal of Mass Compounding Clearances: The FDA proposed excluding semaglutide and tirzepatide from the 503B bulk drug substances list. Approved brand-name medications are no longer facing severe national supply shortages. Outsourcing facilities cannot lawfully compound copies without a recognized clinical need. This administrative change curtails the legal mass production of low-cost alternatives.
- Crackdown on Telehealth Promotion: Federal authorities issued warning letters to 30 prominent telehealth platforms in early 2026. These companies made misleading claims regarding unapproved compounded formulations on their websites. Some firms hid sourcing data or implied their products matched approved brands. This aggressive enforcement prevents easy digital access to unregulated alternative copies.
- Heightened Risks Driving Rationing: Regulators published specific safety warnings regarding warm shipments and improper cold chain storage. Fraudulent compounding labels and false pharmacy addresses have also been discovered recently. These quality concerns leave cash-paying consumers with fewer reliable local sourcing options. Patients frequently resort to GLP-1 microdosing in 2026 to stretch expensive brand-name pens.
- Transition to Strict Dosing Realities: The market transition forces a sudden return to traditional commercial prescription channels. Unapproved copies do not undergo rigorous federal evaluation for safety or quality. Adhering to strict FDA compounded medication rules removes baseline alternative options. Patients must now look for standard clinical treatment pathways or financial relief models.
What GLP-1 Microdosing Really Saves
Rationing your weight management medication alters your short-term out-of-pocket expenses. Patients calculate microdose semaglutide cost factors by dividing their weekly baseline consumption rates. However, separating immediate financial numbers from actual therapeutic outcomes reveals a distinct financial contrast.
| Expense Category | Prescribed Standard Regimen | Independent Microdosing Regimen |
|---|---|---|
| Upfront Out-of-Pocket Purchase | High initial retail cost per brand-name injection device. | Identical upfront retail cost for the initial brand-name device. |
| Monthly Treatment Consumption Rate | Uses a complete pen or vial supply every 28 days. | Stretches a single pen device over multiple months. |
| Clinical Value and Medical Return | Matches data-proven metabolic thresholds from clinical trials. | Fails to achieve validated clinical thresholds for weight management. |
| Real-World Therapy Persistence | Follows supervised healthcare provider alignment and progress tracking. | Leads to high long-term discontinuation rates and poor adherence. |
| Secondary Expense Risk Profile | Managed under professional medical guidelines to reduce complications. | Risk of sudden weight regain, wasted medication, or hospitalizations. |
← Swipe to see more →
Independent rationing creates a false economy for your long-term health budget. Standard chronic weight management treatments require consistent, predictable concentrations to alter metabolic processes effectively. Real-world health data published by the National Institutes of Health reveal poor therapy persistence among adults using commercial insurance. Approximately two-thirds of tracked individuals fail to remain persistent with their treatment within the first year. Only 27.2% of individuals achieve a true adherent status when modifying their routine away from prescribed instructions.
Paying a reduced monthly rate for a subtherapeutic amount degrades your medical progress. When you drop beneath approved starting limits, your body loses the necessary glycemic and appetite control protections. Discontinuing or fragmenting your treatment plan directly correlates with rapid weight regain and stalled progress. This outcome transforms your calculated financial savings into a net financial loss, as you continue paying out-of-pocket for an ineffective clinical strategy.
Alternatives Patients Explore Instead of GLP-1 Microdosing
Patients look for valid medical frameworks instead of dividing or stretching their doses. Legitimate structural coverage options exist within the United States health system.
Commercial Insurance Appeals and Formulary Exceptions
Commercial insurance coverage limitations trigger a high rate of initial coverage blocks. Consumers can formally contest a GLP-1 insurance denial through established administrative steps. Your prescribing physician must provide a detailed medical statement to support this request. This statement must prove that the requested brand-name treatment is clinically necessary.
Medicare and private plans divide therapeutic choices into distinct cost tiers. Lower tiers carry lower copayments, while higher tiers impose steep expenses. Patients can request a specific tiering exception from their plan sponsor. A tiering exception allows you to pay a lower cost share configuration. Prescribers must demonstrate that alternative lower-tier drugs would be entirely ineffective.
Utilization Management Exceptions for Standard Access
Insurance providers apply utilization management protocols to control active prescription volume. These rules include step therapy requirements and explicit quantity limits. Step therapy forces individuals to try cheaper covered drugs first. You can request a direct exception to bypass these preparatory steps. Your doctor must show that the cheaper drug would cause adverse health effects.
Quantity limits restrict how many doses you can receive per month. If your medical condition requires a distinct amount, exceptions are possible. Overcoming these blocks guarantees access to a full, standard therapeutic dose safely. It removes the pressure to stretch existing medications independently without supervision.
The 2026 Medicare GLP-1 Bridge Initiative
Federal coverage pathways are changing significantly for elderly and eligible U.S. patients. The Centers for Medicare & Medicaid Services introduced a major structural update. A voluntary model named the BALANCE Model was announced to expand access. This framework combines negotiated medication access with data-verified nutrition supports.
A temporary payment demonstration serves as a direct preparatory bridge. The Medicare GLP-1 Bridge officially begins operation on July 1, 2026. This program operates outside traditional Part D risk-sharing flows. It runs through December 31, 2027, to enhance affordability options. Eligible individuals enrolled in Medicare Part D receive predictable baseline pricing thresholds.
Affordable Federal Copayment Structures
Eligible beneficiaries face vastly reduced out-of-pocket spending under this framework. Under the federal demonstration, patients pay a fixed 50 dollar monthly copayment. This covers a full month's supply of approved weight management medications. The centralized processor manages prior authorization and pharmacy claims adjudication directly.
Specific National Drug Codes define which products qualify for this bridge. Beginning July 1, 2026, all formulations of Wegovy are fully accessible. All formulations of Foundayo are also included in the approved directory. The KwikPen formulation of Zepbound qualifies for the flat 50 dollar price. However, single-dose vials and single-dose pens of Zepbound are excluded.
Manufacturer Direct-Pay and Assistance Programs
Pharma producers operate independent financial safety nets for non-Medicare consumers. Eligible commercial or uninsured buyers can research a manufacturer's direct-pay program. Brand-name firms provide direct savings cards to reduce retail pharmacy burdens. Hardship programs like Lilly Cares also provide clear assistance based on income.
These programs offer high financial value if you lack comprehensive insurance. They provide legitimate access pathways to fully sealed, regulated injection devices. Utilizing these systems eliminates the calculation errors linked to unofficial click charts. It keeps your treatment plan aligned with safe federal manufacturing requirements.
Regulated International Pharmacy Sourcing
Consumers frequently analyze international therapeutic supply networks to bypass high local pricing. Searching to buy Ozempic online in Canada serves as a common alternative path. Verified Canadian operations dispense identical brand-name medications under strict local health rules. This structure avoids the safety hazards linked to warm telehealth compounding shipments.
International procurement allows cash-paying buyers to maintain prescribed titration schedules. It delivers a full, unadulterated supply to your doorstep through coordinated logistics. Patients receive proper temperature-controlled packaging to protect chemical stability. This structural solution secures treatment consistency without compromising your physical well-being.
The Bottom Line: Is GLP-1 Microdosing the Best Saving Strategy for You?
Independent dose reduction fails to deliver the medical benefits proven in clinical trials. Rationing your injections to lower expenses creates a false long-term economic model. Fluctuating active levels disrupt metabolic stability and frequently trigger sudden weight regain.
Seniors and commercial buyers can access standardized care through verified legal programs. Securing fully sealed, authentic therapeutic supplies protects your long-term health outcomes. Reviewing established global supply channels ensures affordable management for metabolic and chronic conditions.
Frequently Asked Questions
No. Comparing microdosing GLP-1 vs. regular dose schedules shows that standard dosing achieves proven metabolic thresholds. Microdosing operates completely outside approved clinical guidelines. Subtherapeutic amounts often fail to deliver consistent or meaningful weight management results.
Gastrointestinal issues are the most frequent adverse events. Patients commonly report severe nausea, vomiting, diarrhea, and abdominal pain. While some users try microdosing to manage these symptoms, medical professionals recommend following an approved standard therapeutic dose escalation.
Federal regulators have not approved fractional dosing protocols for these medications. Manual extraction or unapproved dose adjustments significantly increase the risk of serious dosing errors. The FDA warns that improper measurement can lead to adverse events requiring hospitalization.
Discontinuing weight management medications typically causes rapid weight regain. Clinical data indicate that stopping GLP-1 therapy reverses the metabolic and physical progress achieved during treatment. Maintaining a consistent, data-proven regimen is necessary for long-term success.
Many patients utilized unapproved copies during the compounded GLP-1 shortage. However, recent FDA compounded medication rules strictly limit this practice. Outsourcing facilities cannot lawfully mass-produce these alternative copies when approved brand-name drugs are commercially available.
If you experience a GLP-1 insurance denial, you have valid structural alternatives. You can apply for a manufacturer direct-pay program to lower your out-of-pocket expenses. Elderly patients will also soon benefit from expanded Medicare Part D GLP-1 coverage through new federal bridge programs.
Disclaimer
This blog is provided for informational purposes only and does not replace professional medical, insurance, financial, or prescription guidance. Pricing, availability, prescription requirements, shipping timelines, and medication access policies may change over time and vary by provider, pharmacy source, and insurance plan. Always consult your healthcare provider, insurance representative, or official government resources before making medication, prescription, or coverage decisions.





